For our latest Notable Narrative we chose Kevin Sack’s “60 Lives, 30 Kidneys, All Linked,” a New York Times story about an unprecedented chain of kidney transplants. We admired the story as a deft and moving example of explanatory narrative, and because Sack, a two-time Pulitzer winner, chose an unlikely protagonist, with deeply touching consequences. How did he pull it off? Here’s our recent telephone conversation, edited for length and clarity:
You were dealing with a huge amount of complicated information. Could you talk a bit about how you organized it, and how you presented it in such a graceful, moving way?
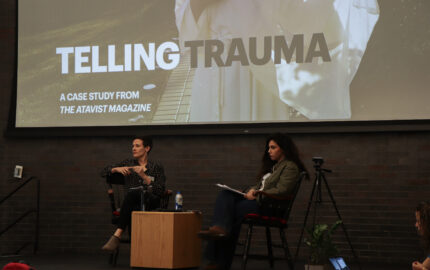
To report “60 Lives,” the New York Times’ Sean Patrick Farrell, Kevin Sack and Nicole Bengiveno scrubbed in for surgery after surgery.
It sounds a little silly to say that a story like this wrote itself, but to some extent the material was so compelling that it made the job a little bit easier. There were certain things that I knew were going to have to be included in the roughly 5,000 words I was allotted. Pretty much from the beginning I felt there was going to be a certain logic to writing it in a roughly chronological way, or at least with an emphasis on the first link in the chain and the last link, and with the rest of the story composed of equal parts explanation of how the chains work – the medicine, and what I witnessed in the operating rooms – and the history of these chains, and the best human stories that I could find from within the chain. Before I started reporting, I assumed that at every link there would be a great narrative tale. By definition there had to be: Somebody’s giving up a part of themselves for a loved one. How uninteresting could it be? The challenge was gonna be to find out about as many of those links as possible in the time allotted, given the other things I was going to have to accomplish, and then picking out the best tales. When you look at the story there’s only a handful of stories in it, out of the 30 transplants. There were a lot of great stories left on the cutting room floor on this one, sort of by necessity.
The biggest decision I had to make in terms of how to structure and write it – I longed to simplify the story by focusing on a smaller number of people. I was concerned all along that even if I minimized the number of characters there would be too many characters. I didn’t want it to get bogged down in a long list of names. People wouldn’t be able to keep it straight. And the stories would start to dilute each other. Ultimately I decided that that was wrongheaded.
What do you mean?
The central character was the chain itself. And by definition the chain consisted not of a handful of people but of 60 people. What made it miraculous was that there were 60 participants and that these kidneys flowed relatively seamlessly from one link to the next. And so I decided that to focus on a central character kind of undercut what the story was all about. Once I wrapped my head around that, I think I got more comfortable with the notion of doing it the way I did, with a number of central characters. I kind of dip in and out of each of their tales rather quickly, mainly because I have to. As I was reporting the story, Amy Harmon’s great piece about the autistic couple in love ran, and I was envious because she was able to tell a story that essentially was about the socialization of autistic people through the eyes of a single couple. I was a little jealous and wanted to find a way to do that, but then quickly decided that the point of the (kidney) story is that there were 60 characters, not that there were two.
Where did this story come from?
I’m certainly not the first person to write about these chains. There was a New England Journal of Medicine article in, I think, ’09 that was about the first of these chains that were structured this way, with a Good Samaritan starting a donation to the waiting list and then non-simultaneous operations. So there was a flurry of stories after that, about these chains. I was covering Obamacare at the time. We were sort of in the thick of legislative battle, and it wasn’t something I was going to be able to get to at that point but I filed it away as being interesting.
I had a change of jobs back in the fall, where I got assigned to this new team of reporters created by Jill Abramson to doenterprise stuff on lifestyles. It was sort of broadly defined, and my part was that I going to continue to write about health-related issues. I had a list of story ideas that I put in front of my new editor, Adam Bryant, and he quickly got interested in the kidney-chain story. So I went out to see sort of what had been written, whether there was any room left to do something interesting, looking for, you know, an angle that would sort of give us a reason to do it, and to do it in a big way. My third or fourth call was to Garet Hil, whom I’d started to hear about and read about. He was in the middle of what was going to be the longest chain ever constructed. So I suddenly had my angle. I took it back to Adam and to others at the paper and there was a lot of enthusiasm about it and resources put into it quickly.
Such as?
A very quick decision to make it a big multimedia project. So: photographers assigned, graphic artists assigned, interactive designers assigned, a video journalist assigned. And sort of involvement from people on the masthead at the paper in terms of getting their attention and early signoff, an assumption that we’d probably do it at two pages long. All those things were in place pretty quickly.
Where in the chain was the transplant process at that point?
They were exactly halfway through. I found out about it in early November, and they were in the middle of this long bridge, as they call it, between donations. This was a point where a recipient had been transplanted – their paired donor had yet to donate, typically for some sort of logistical reason. This was the longest pause in the chain. It was from I think late September to early December, almost two months.
Which people in the chain? Could we look at it that way?
Identify which ones?
Yeah.
I think it was No. 16, Rebecca Clark. Yeah. John Clark, No. 15, had received his transplant, and his wife, Rebecca Clark, did not donate until Dec. 5. He had been transplanted on Sept. 28. My initial concern was, Well I’m not gonna be in on the beginning of this and that’s gonna be awkward, to do a narrative that way, because I’m gonna have some stuff that’s much more vivid than the rest of it. In retrospect, I think it ended up being an advantage. First of all, it cut the time of the project in half. For a project like this it was relatively quick: 3 1/2months from conception to publication.
Wow.
And also, it made what I did see fresher, I think. It wasn’t that difficult to go back and reconstruct the first half of it. And the timing worked out kind of just right, because once I found out about the chain from Garet it gave me a month to get my ducks in a row before surgeries actually started again. So I was able to spend that time reconstructing the first half. I went to New York and spent a day with him at his office on Long Island. I interviewed a lot of doctors and people in the field, read a lot of journal articles, and also was able to get the rest of our team up and moving. They started collecting names and IDs and photos of people in the first half of the chain. Which was a process. So the timing worked out nicely.
I spent most of December kind of running. We had a sort of interesting decision to make: We had a meeting in New York with all the people involved – we had to make decisions about where we were gonna go in terms of actually being at the hospital and watching procedures and interviewing patients. Part of that was gonna be driven by who we thought was interesting given what I knew at that point about the chain, and part of it was gonna be driven by pure logistics. I knew that I wanted to be present for the end of it because I was going to highlight the last recipient. And there also was this great flurry of procedures on the penultimate day at UCLA. There were six surgeries from dawn to dusk that day. So I figured that would be a great place to be, and then fly with the last kidney to Chicago for transplant. But I was worried that what if the chain breaks before we get there, which definitely was possible.
One of the first things I did the first month was, Garet shared all the emails that he sent and received relative to the first part of the chain, and you could see all these different points where things had broken down for one reason or another, and he had had to repair breaches. So I knew that this chain that’s supposed to be 30 transplants long could end up being 17 transplants long and if I was going to be there for the last three or four I’d have nothing to write about. So we decided to pick a surgery early in December, when the chain first started back up, to go and eyewitness, and to focus on those participants so that if disaster struck we’d have something.
I don’t know if you’ve looked at all the stuff online or not –
It’s killer.
We ended up doing a video piece about Cesare and Josephine Bonventre – he’s from Brooklyn, she’s from Toronto, they’re mentioned briefly in the print story because they’re the only example in the chain of a compatible pair, meaning she could’ve donated to cousins, she could’ve donated directly to him, but by donating down the line instead he was able to get an even better matched kidney. Which is kind of the next wave in these chains: It expands matching potential by including compatible pairs. So the day before the surgery I went with a photographer (Nicole Bengiveno) and videographer (Sean Patrick Farrell) to his place in Bensonhurst and interviewed the two of them at length, went with him to his final dialysis treatment at a clinic in Brooklyn – again, with cameras in tow – and the next morning we all showed up at the hospital at 4:30 in the morning and watched them from the beginning of the day to the end of the day, including both their surgeries. Then we had something in the can that we could use to construct the story if we had to. They’re sort of highlighted on the interactive graphic.
It’s great to work with them. It’s real value added to what we do, particularly for a story like this that’s so graphic in nature.
The permissions on this must have been tricky, getting all 60 to participate – well, 59 – for their names to be used, for their photographs to be used. How did you handle that logistically? And why didn’t that 60th person, the one in silhouette in the grid, want to do it?
HIPAA obviously prohibits hospitals from releasing these names or anything about these folks without their express permission in the form of a signed, written waiver. There are 17 hospitals involved. So I went to each of the hospitals. From Garet, I had sort of a spreadsheet that showed the course of the chain with some detail: the gender of the donor and recipient, the year of their birth, a code name – no real names – and the hospital that they were gonna be at on the day of the surgery. That’s pretty much what I had. So I was then able to go to the hospitals, explain the story to them, get them to go to the patients, get the waivers and then put me in touch with the patients.
Wait a minute, though. It’s a miracle that you got any of these people, much less 60. Anytime you have other people asking permission for you, you know how that goes –
Right. The one advantage that I had in this case was that the people doing the asking had incentive to get people to yes.If they got people to yes it meant that their hospital might be mentioned in the story. And these were the PR people who were usually involved. So most of the hospitals were eager to pursue it. And I obviously did some coaching, to fully explain the story to people and what we were doing and how the information would be used. The other advantage that we had, a lot of people who go through this process become real zealots about it – they want to spread the word. They feel that they’re saving lives and that (Good Samaritan donation is) an underutilized strategy and if more people knew about it more lives could be saved.
The person that said no was one of the first that I pursued, because I was basically going in order. I called this hospital in New Jersey, Saint Barnabas, and they were just sort of stunned that this person had declined. They thought maybe he was just having a bad day. They thought it was uncharacteristic and unexpected that he would say no, so I sort of maintained hope. We continued on and you can imagine what it’s like – it’s sort of clerical. You send out these requests and some come back pretty quickly and others you have to follow up on three and four times and eventually they started to come through. But yeah there are 59 pictures and one blank.
It does speak to some people’s reluctance and fear about this whole thing –
Right. I mean, obviously I have no sense for his reasoning for not wanting to disclose. It could be any of a number of things; I respect all of them. I was surprising that such a high percentage of people were willing to put their names and faces out there. Sometimes people just don’t want others to know that they’ve been ill or – I mean there are all kinds of reasons for them to not join in. They just cherish their privacy and understandably so. But there was a bit of a mission-oriented feeling for this, I think, for a lot of the participants.
Beautiful writing. There’s this one sentence: “On and on the chain extended, with kidneys flying from coast to coast, iced down in cardboard boxes equipped with GPS devices and stowed on commercial aircraft.” That’s a whole procedure that you just managed to collapse as one gorgeous sentence. You’ve collapsed time, you’ve made procedure easy for the reader to follow.
one of Sack's notebooks
One thing I did that I don’t always do, even for long narrative projects like this, is, I outlined. I sort of methodically over a period of days went through my notes, kind of made a list of key points and key scenes and key characters, and then roughly organized them. And pretty much followed that structure. It certainly was deliberate, to try to write it in a restrained manner because the material itself was so strong and emotional and so potentially prone to purple prose. You do enough of those and you come to realize that if your material’s good enough you just don’t need to overwrite it. Not that there’s ever a reason to overwrite anything, but you know what I’m saying. Beyond that, I really do feel like I just sort of followed the outline and constructed these scenes. I had to show discipline in terms of what we included and excluded. The original draft was not that much longer than the final one – I think just a few hundred words, and lots and lots of editors touched it before it got in the paper. I must say, all made really good suggestions and improved the story.
There’s one interesting tale about all this. The last line of editing is (Executive Editor) Jill Abramson. On the Friday before publication – and I think it was the Friday that she was rushing out the door to fly to Beirut to console Anthony Shadid’s widow and children – but before she got on the plane she ordered that I change the kicker on the story.
Oh!
So here we are, it’s been through umpteen levels of editing at this point and everybody’s signed off on it, and the executive editor is ordering up a change at the last minute. The issue was – the initial kicker had to do with this story that the final recipient, Don Terry, tells, that I just found irresistible, about how in late November, before he knows that he’s getting this kidney, he’s out with his cousin and her two young children, and they go to this sporting good store because they know Santa is gonna be there for photographs with kids. And the kids get on Santa’s lap and then as a goof Don and the cousin get on Santa’s lap and Santa says, “So, young man, what do you want for Christmas?” And Don says, “Well, Santa, the only thing that I want is a kidney. That’s all I want.” And Santa sort of plays along, looks him in the eye and says, “I think you’ve been a good boy this year. I think you’re gonna get that kidney.”
Ugh.
And two weeks later he gets the phone call from the transplant surgeon saying: “You’ve got the kidney.” Jill thought it was too much, that it was over the top and melodramatic, even though it happened and was real. Her point was exactly yours. The rest of the story had been written in this restrained sort of underwritten way, to some extent, and this was going to be jarring to the reader. This was all communicated to me through deputies but I think her sense was that I’d just sort of gotten to the end and I just couldn’t help myself.
(laughter)
I just couldn’t get all the way through without letting one rip.
That’s awesome.
So I sort of resisted and kicked the dirt a little bit, but in the end it didn’t matter because she’s the executive editor and I’m not. But in retrospect I think she was probably right.
I think so too.
And we found a decent alternate.
You found a great alternate. It’s forward-looking, whereas a Santa ending would’ve been a dead end.
I hate to say it but sometimes the executive editor of the New York Times can be a smart person.
So, the response to this piece – what has been the impact so far?
Well, they got a nice surge of offers of Good Samaritan donors both at the National Kidney Registry and at transplant centers individually. The National Kidney Registry had 426 donor registrations, Good Samaritan donors, in February, when the story ran. That compares to 120 in January, 81 in December, 79 in November, 70 in October. And then they had 300 patient referrals to member centers. These are patients coming in with paired donors, and that was more than three times the usual number. There was lots of sort of media follow-up. Diane Sawyer did a big piece on ABC. Lots of local TV. BBC did a piece.
And then there was a recent conference involving the debate about whether to create a national registry.
There was this consensus conference near D.C. where a bunch of specialists got together – surgeons, transplant coordinators, nurses, patients, insurers – to discuss the future of the field and look at ways to increase the number who get transplants this way. One of the key things on the table is whether there should be a single national registry, which the mathematicians and to some extent common sense tell us would presumably increase the number of transplants made possible. The bigger your pool the more potential matches you can make. A committee of this group recommended doing exactly that, which for the moment is likely to mean exactly nothing. It’s purely a recommendation. It’s a sense of direction of a committee of this group.
There’s a lot of transplant politics involved. These different registries compete with each other. They have different philosophies. They’re all virtually unregulated by the government at this point and there’s nothing constraining them from operating the way they want to. It’s not my sense that there’s going to be much change anytime soon. Garet Hil, the guy that’s featured in my story, has the most successful of these registries and he doesn’t see much of a reason to change the way his is working. He feels like he’s got a model that’s getting transplants done, and he’s concerned that any sort of merger, particularly a merger that puts him more at the mercy of government regulation and oversight, is going to decrease the number of transplants he can accomplish.
Speaking of Hil, this isn’t a traditional narrative in that we’re not following one or two main characters, we’re not using a ton of dialogue, but you are following, as you said, the arc of the chain itself and then looking at these little narratives along the curve. But there’s this sort of overarching hero in Hil – the former Marine recon ranger with a background in quantitative math, who started the registry after his own kid got sick. Another writer might’ve decided that that guy was the narrative and folded the chain around his story. It was a riskier and much more complicated piece of storytelling, what you did.
I think I was driven by my interests – and they were varied – in this subject. I was completely captivated by him. I think he’s a fascinating guy. But I thought there were other fascinating parts to the chain. And to some extent, because he very much deliberately distances himself for ethical and legal reasons from the participants in the chain, if the story had focused more on him it would’ve been at the cost of the other parts of the process, which were all pretty darn compelling. I mean, until I wrote the piece he didn’t have names for these people, for the most part. So more of a focus on him would’ve meant it would’ve been harder to humanize the chain. It would’ve been more about the math of what he does and his personal story.
When you described him as “Disney-hero handsome” which Disney character did you have in mind?
The one that I really had in mind – it ends up being the wrong one to have had in mind because as I thought about it more, he’s not a hero, he’s an oaf. In “Beauty and the Beast” I’m thinking Gaston, who is Belle’s pursuer. I’m extremely familiar with the story right now because I’ve just watched three performances of my stepdaughter in a middle-school production. But yeah, he’s got the same sort of cleft chin. Lots of hair. And he’s not heroic at all – he’s an anti-intellectual. Surely there were other heroes. Prince Eric maybe? In “The Little Mermaid?” I don’t know. Don’t you find Hil Disney-hero handsome?
Uh-huh.
He’s happily married.
Good for her, is what I can say about that. I love how you de-glorified Ruzzamenti by mentioning his carousing, and his “unsmiling presence at work,” and his “surliness,” and his inattention to his parents and grandmother. He’s real.
That’s what I loved about him. He’s such a quirky guy and would be the first to tell you so. We had a really good time interviewing him. I talked to him a couple of times by phone and then spoke to him at his home when we flew out to UCLA for the last part of the chain. He lives in Riverside, which is an hour or two away, so it was convenient. He’s just a real character. I’m not sure that I give the reader a real way to understand him because I’m not sure that I completely understand why somebody, who by his own admission may not be the sunniest or most giving person every moment of every day, becomes an incredibly giving person at this one moment.
Maybe it’s redemption. Maybe if you’re an ass your whole life and you get the chance not to be, you take it.
Yeah. I think there’s certainly – he didn’t want me to overemphasize the notion of his Buddhism and its impact on his decision, because I think he feels he had this in him before he discovered Buddhism, but there’s a certain karma for him. I don’t think he felt, “I’m gonna go do a good thing and it’ll pay off in the next life,” but I do think he has a sense that the good things you do in life at some point have an impact.
The play-by-play of Conor Bidelspach’s kidney removal was so descriptively written: “The slush in the blue bowl turned fruit-punch pink.” And you wrote about a plastic bag knotted shut “like a goldfish brought home from the pet store.” Clearly you’re the father of young children.
(laughter)
You were there for that, though, obviously. You scrubbed in?
Yeah, from beginning to end I saw six different procedures at three different hospitals: the nephrectomies, which is the kidney recovery, and then the transplants. In each case I had photographers and video journalists in the O.R. with us. We scrubbed in, we were in scrubs, with masks and hairnets and note pads and cameras. The doctors seemed to be completely unfazed by the fact that we were there. They’ve done the procedure 100 times a year. And I think two of the hospitals required that we have TB tests. One of them required us to sign various waivers in case there was any havoc in the operating room, any trouble that we caused. But it was all fairly smooth. We just sort of took turns stepping up on a little stepstool just behind the surgeons, peering over into the abdomens as they did their work. With the nephrectomies, there were these screens all around the operating room, showing what’s going on, because it’s all done laparoscopically and there’s cameras inside the cavity, showing what’s happening.
Interesting that you wrote that someone “poured” a kidney. Interesting verb.
I’ve got this vague recollection that that wasn’t the first word I used. An editor may have come up with that choice. I may have said “emptied” or something like that.
“Poured,” with reference to a human organ, is odd in a good way. Unexpected in a good way.
It definitely helped to see the procedures multiple times. The first time out you’re just sort of absorbing it and each time you see it you may think a little more in metaphor and imagery.
Getting back to a conversation you and I were having earlier: We were talking about long-form narrative versus daily reporting.
I’ve never seen the disconnect between hard news writing and narrative reporting and writing. I try to use the same skills. If I’m covering a hard-news story I’m looking for the same narrative elements and the same imagery and the same way of describing something metaphorically that I would when I’m reporting a narrative. I mean, I have the same opportunities to use it, depending on the story and how much space I’ve got. It’s always seemed to me that even the hardest news story is helped by narrative elements. Obviously you deal with them in different ways depending on your format. But I’ve just never seen the distinction. Both ways of telling a story are equally credible in terms of getting at the truth, which is ultimately our goal and our mission.

 I’ve never seen the disconnect between hard news writing and narrative reporting and writing. I try to use the same skills. If I’m covering a hard-news story I’m looking for the same narrative elements and the same imagery and the same way of describing something metaphorically that I would when I’m reporting a narrative. I mean, I have the same opportunities to use it, depending on the story and how much space I’ve got. It’s always seemed to me that even the hardest news story is helped by narrative elements. Obviously you deal with them in different ways depending on your format. But I’ve just never seen the distinction. Both ways of telling a story are equally credible in terms of getting at the truth, which is ultimately our goal and our mission.
I’ve never seen the disconnect between hard news writing and narrative reporting and writing. I try to use the same skills. If I’m covering a hard-news story I’m looking for the same narrative elements and the same imagery and the same way of describing something metaphorically that I would when I’m reporting a narrative. I mean, I have the same opportunities to use it, depending on the story and how much space I’ve got. It’s always seemed to me that even the hardest news story is helped by narrative elements. Obviously you deal with them in different ways depending on your format. But I’ve just never seen the distinction. Both ways of telling a story are equally credible in terms of getting at the truth, which is ultimately our goal and our mission. I’ve never seen the disconnect between hard news writing and narrative reporting and writing. I try to use the same skills. If I’m covering a hard-news story I’m looking for the same narrative elements and the same imagery and the same way of describing something metaphorically that I would when I’m reporting a narrative. I mean, I have the same opportunities to use it, depending on the story and how much space I’ve got. It’s always seemed to me that even the hardest news story is helped by narrative elements. Obviously you deal with them in different ways depending on your format. But I’ve just never seen the distinction. Both ways of telling a story are equally credible in terms of getting at the truth, which is ultimately our goal and our mission.
I’ve never seen the disconnect between hard news writing and narrative reporting and writing. I try to use the same skills. If I’m covering a hard-news story I’m looking for the same narrative elements and the same imagery and the same way of describing something metaphorically that I would when I’m reporting a narrative. I mean, I have the same opportunities to use it, depending on the story and how much space I’ve got. It’s always seemed to me that even the hardest news story is helped by narrative elements. Obviously you deal with them in different ways depending on your format. But I’ve just never seen the distinction. Both ways of telling a story are equally credible in terms of getting at the truth, which is ultimately our goal and our mission.