As a writer who routinely embeds in her subjects’ lives, the COVID pandemic was a blow to Lane DeGregory’s reporting. She was barred from sit-down interviews, where she would normally run through a list of 30 quasi-psychoanalytic questions. Even when she could be present with her sources, masks obscured their faces. The lack of handshakes and hugs felt weird.
DeGregory, who has worked at the Tampa Bay Times (formerly the St. Petersburg Times) since 2000, is known for her intimate narratives that illuminate, as she puts it, “people in the shadows.” Her bylines include the 2009 Pulitzer Prize winner in feature writing, “The Girl in the Window,” a portrait of a family’s adoption of a feral child. She recently completed an expansive series profiling cadets in their six months at the police academy.
For 18 months, DeGregory found other ways to document the ways the pandemic was whiplashing her Florida community. She shadowed a hospice chaplain who held patients’ hands when their families were locked out of hospital rooms, and visited a 96-year-old who continued to operate her state-designated “essential” business (a liquor store).
But a critical angle was missing, DeGregory remarked during an April 2020 episode of the podcast “Write Lane:” Where are the stories from inside emergency rooms and COVID wards?
DeGregory contacted facilities every few weeks.
“I’ve tried at least a half-a-dozen different ideas and at least that many institutions for each idea, and we can’t get in,” she told her listeners back then. “It’s been really, really frustrating to not be able to tell those front-line stories.”
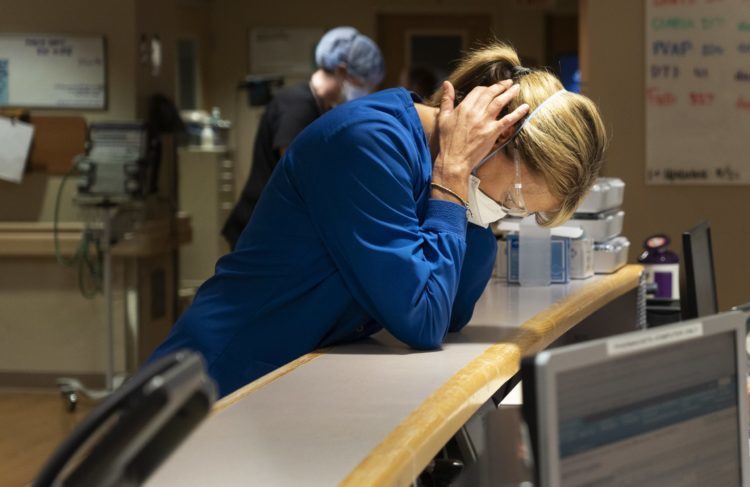
How then, did DeGregory ultimately gain entry to a COVID-19 intensive care unit, where she and photographer John Pendygraft shadowed a nursing supervisor through a 12-hour shift?
The resulting story, “Twelve hours in a Florida COVID-19 ICU,” published on Sept. 2, 2021, is a case study in flexibility and compromise. DeGregory said the article was one of the “hardest” and “saddest” she has undertaken in a 30-year career of doing hard, sad stories.
“You’ve got to keep asking.”
“We are bound by very significant federal privacy laws about health care information,” Joni James told me. She’s the director of communications at BayCare Health, which runs 15 hospitals in west-central Florida. “Our job is always the patient first. Any story that we’re going to tell, it has to serve that or it has to serve the community’s health.”
It is worth noting that James previously was the Times’ deputy editorial page editor at the Tampa Bay Times, She and DeGregory are friends. But that wasn’t enough to grant DeGregory’s requests for access.
Then, this past summer, the Delta variant launched its insidious march across the U.S. By mid-August, Florida was a hotspot for new infections, with a seven-day average of 21,000 cases. Increased hospitalizations and deaths followed, mostly among the unvaccinated. In Tampa, ambulance crews waited in lines to deliver patients to overrun emergency rooms. Hospitals canceled elective procedures. State political leaders, notably Republican Gov. Ron DeSantis, continued a campaign to block the power of municipalities, school districts and businesses to implement vaccine and mask requirements.
DeGregory pressed her case again.
“You get told ‘no’ every day, but you’ve got to keep asking,” she said during a recent interview.
And this time, with vaccinations stalled and the situation dire, BayCare said yes.

“We became aware that people in our community didn’t know what the Delta variant meant in terms of the new surge in cases,” James said. “So many of the people in our care were unvaccinated. We really felt it was a public service to pull back and make people aware of the dangers of COVID.”
She also noted that knowledge of the virus had progressed to the point where hospitals could safely admit visitors, including journalists. But as important was DeGregory’s reputation for fair and empathetic storytelling.
“She asks a lot of questions, rather than assume,” James told me. “Trust is required in these situations. You need to be able to trust that this person is able to bear witness. This isn’t accountability journalism. If you want to do the FRONTLINE piece, you probably aren’t going to get inside the door.”
James helped arrange DeGregory’s visit with Jennifer Tellone, the nursing supervisor at Morton Plant Hospital in Clearwater, Fla. The hospital provided a brief pre-interview the day prior. But conditions were set.
“I would have gone home with Jen,” DeGregory said. “I wanted to see her take her shoes off and put them in the trunk, greet her husband and her dogs, and see her kids.
“But I wasn’t allowed to. I was also told I was not really allowed to talk to Jen during those 12 hours because I couldn’t get in the way, which I understand. I was very grateful for what we got — that we got anything at all.”
Four days from notebook to press
DeGregory’s day began in the hospital lobby a little after 5:30 a.m., just before the start of Tellone’s shift. DeGregory and Pendygraft were vaccinated and wore N95 masks.
As she worked, DeGregory enlisted her wartime muses, “M*A*S*H” and the late Ernie Pyle. She filled a legal pad, which is her go-to notebook, with rare treasures: firsthand sensory details like the clicking and beeping of monitors; moans of suffering patients, and the incessant spinning of blue lights that announced someone had coded. In her story, the pathos builds with each haunting scene, but there is an absence of catharsis.
DeGregory, who has earned major awards for her long-form projects, often still works under intense deadline. She said editors at the Times feared her piece would lose its urgency if Florida’s crisis eased. They gave her four days to turn in a draft.
“You write it in such a hurried manner — and walk away with second-guessing and regrets,” she said. “For the next four or five days, you’re like ‘Oh I wish I had’ or ‘I should’ve, could’ve’ or ‘Why didn’t I?’”
A week after “Twelve hours in a Florida COVID-19 ICU” was published, President Joe Biden announced a federal mandate requiring employees at most hospitals to be vaccinated. That same day, BayCare reported its intent to follow the mandate.
I spoke to DeGregory about the logistics of reporting her story, negotiations with administrators, and the pressure of being one of a select number of reporters to gain access to a COVID unit. Our conversation has been edited for length and clarity, and is followed by an annotation of the story.
Can you describe what it was like reporting from inside the ICU and some of the ground rules you agreed to?
The walls of the room were glass, so we did all the reporting from the hall looking through the glass. We didn’t go in the patient rooms at all, but you could pretty much hear them through the door. Jen (Tellone) moved from room-to-room, and we were allowed to walk around the ward. I interviewed a bunch of other doctors and nurses to get a sense of things.
PR staff shadowed us the whole day, making sure we didn’t go anywhere we weren’t supposed to go or ask something we weren’t supposed to ask or talk to someone we weren’t supposed to talk to. They were kind of like fixers, but they were also blockers. I asked Jen if I could get her personal email and cell phone, and the PR woman jumped right in and said, “No, you’ll have to go through me,” before Jen could even answer.
Jen had a tiny office right off of the ward and at the end of the day she was kind enough to give us an hour to ask a bunch of follow-ups. That night, of course, I had another 70 million questions so I typed them all out for the PR lady and asked if I could call Jen. She was like, “Nope, but I’ll try to get what I can.”
Did you enter this project with a predetermined theme you hoped to explore? And who was your intended audience?
It was just “Let’s put people on the front line and see what these nurses are seeing.” I wanted to take readers to a place to make them feel the impact of what was really happening. I want to show people this is real and not fake news. I want to get beyond numbers and pie graphs. What if you were Jen for a day? I wanted to write for readers who weren’t going to see that for themselves.
The themes we talked about were frustration, desperation and helplessness.
How did you obtain background information on the patients? Were you allowed to talk to them?
No. But during rounds, outside every patient’s room, they would summarize: “Room 84: This is a 56-year-old man from Brandon, Fla., who came into the regular hospital on Aug. 3. He’s been with us for four days now and his blood sugar is high and he is desaturating and he needs to be put on a ventilator.” They would give that little thumbnail of every single patient.
One of the respiratory therapists and a nurse were hanging back, taking notes. They were offering other details without us having to ask. Things like: “Oh my God, that poor woman. She just bought a house.”
After the story (was complete), John (the photographer) and I vetted all this stuff with the PR people. We had a phone call with me, Joni James, Maria Carrillo (DeGregory’s editor at the Tampa Bay Times) and the hospital PR person, where she said, “Read us what you say about each patient.”
We had to do this dance step with them about what we could and couldn’t say. It was a lot of work to blur the specifics that normally I would have dived into.
I imagine you in front of your computer after the hospital visit. You need to write. Where do you start?
I got up early on a Saturday and read through my notes and tried to figure out what I was going to do. That’s when I kind of lost it.
It was such a gift being let in there. I felt so much pressure to do a good job. The challenge of trying to find a unique spot in the canon of COVID stories weighed very heavily on me. I’m writing about something that everybody and their brother all around the world has written about for the last 18 months. What can I do to make mine different or better? I don’t want to let the hospital people down or my fellow journalists down or squander the chance that the newspaper finally got. I want to do the best to honor and tell the stories of these front-line health care workers.
I don’t know which of those broke me down, but I just sat there and cried a while before I could start to type.
Annotation: Storyboard’s questions are in red; DeGregory’s answers in blue.

Twelve hours in a Florida COVID-19 ICU
On this ward at Morton Plant Hospital, nurses are overwhelmed by the number of new, desperate cases.
By Lane DeGregoryPublished Sep. 2, 2021 / Updated Sep. 10
She gets to the hospital 20 minutes before her shift, walks through the lobby carrying a smoothie, hoping — but not believing — that today might be better than the day before.
When she steps off the elevator on the second floor, she turns left, toward what used to be the Intensive Care Unit. Since mid-July, it’s become the COVID-19 ICU.
Jennifer Tellone has started calling it “The War Zone.”
In the small office she shares at Morton Plant Hospital in Clearwater, Jen lifts her mask to sip her drink. She hasn’t even put down her purse when another nurse rushes in.
The patient in Room 84 can’t breathe. She needs to be intubated — right away. “Want me to put in for a chest X-ray?” Jen asks, pulling an N95 mask over her surgical one.
“They’re on their way.”
“Is there anything you need me to do?”
“Ask for fentanyl.”
Through the glass wall, Jen sees the patient on her back, gasping, arms flailing. Nurses wearing plastic gowns and respirators are struggling to sedate her. Others are pumping air into her mouth with a plastic bulb.
Tubes snake from her wrists and chest. Above her head, monitors blink green, red and blue lifelines. Outside the door is a cart labeled: “For Code Use Only.”
As you were writing, did you make a conscious effort to avoid medical jargon?Usually, I try to write for the layperson who is not going to have any inside knowledge, but I was so wishing I knew more about medicine and what they were doing. I wish instead of a PR person they could have given us a nurse or a nursing student or someone I could go, “What’s going on? What are they doing?” (I didn’t think to ask for that). The medical stuff was so confusing that I felt completely inadequate. The only way I was able to come to peace with it was to say I’m giving a laymen’s perspective. I’m not giving a medical perspective. I’m only going to give readers what I can get by watching.
The patient is 63 years old, someone reads from a chart. She had been hospitalized two weeks earlier and rushed to the ICU that morning.
“Where’s her family?” asks Jen.
“Her son is here,” says another nurse.
Jen nods, then sighs. “This is how yesterday started.”
Yesterday was the worst day on her ward. Ever. Three COVID-19 patients died — two before 8 a.m.
They were 44, 50 and 64 years old.
Jen had to tell their families.
A man collapsed on the floor beside her, wailing when his wife passed.
A woman begged Jen to save her husband, sobbing, “How do I tell our 6-year-old daughter, ‘Daddy’s not coming home?’ "
Jen is a trauma nurse, mom to two teenagers. She rarely cries.
Yesterday, for the first time in forever, she broke down.
Her husband told her, “Whenever you’re ready to step away, I’ll support you.”
Today, she woke in the dark, pulled on her blue scrubs, tied her hair into a ponytail and came back for a 12-hour shift. She’ll try to save the sickest COVID-19 patients, knowing that no matter what she does, most of them won’t make it — and that so many more are waiting for those beds.
Jen made a career in intensive care because she likes treating a variety of life-threatening conditions, helping the worst patients get better and go home. She’s been a nurse on this wing for 20 years and is now a manager.
When the pandemic hit in March 2020, she helped set up the hospital’s first COVID-19 ward, implementing new protocols. Everyone was terrified, anxious for their patients and themselves.
But by this spring, doctors had figured out new treatments. They had better medicine, new machines. People were getting vaccinated. Nurses began scheduling vacations, wondering when they might be able to stop wearing respirators.
Jen’s unit has 18 beds. In June, there were only an average of three COVID-19 cases each day.
Then, two weeks into July, cases started spiking. In one month, infections increased 10-fold. To make room, BayCare had to suspend elective surgeries in its 14 hospitals across Tampa Bay.
About 40 percent of the beds in those facilities now are filled with COVID-19 cases. On this day, near the end of August, BayCare’s hospitals have 1,164 cases — 462 more than during the peak in July 2020, before there was a vaccine.
Across the country — around the world — the same scenes are playing out. Emergency rooms are overwhelmed. Ambulances are being turned away. More people are dying each day: An average of 250, just in Florida.
The delta variant is spreading faster, striking harder, hitting younger people, even kids.
The saddest part, Jen says, is this didn’t have to happen. Most of her patients, and the ones suffering the most, haven’t been vaccinated.
“How did we get here?” asks Jen, who got vaccinated as soon as she could. “What’s wrong with people who still don’t believe?”
Was there any discussion with your editors about the extent to which the article would draw attention to vaccination without starting to sound preachy?That was a huge factor that I feel you need to convey to readers, but how do you say that without wagging a finger at the victims or the patients? I think I decided to make it a thing through Jen’s eyes because she was kind of incredulous about that. Let her be the one who was outraged.
For her and her staff, last summer’s fear and anxiety have morphed into frustration and anger.
Some patients beg Jen for the vaccine, though it’s too late. Others continue to insist COVID-19 is a hoax — while they’re dying.
Her job is to try to save them, not judge.
But people are suffering so much more, she says, languishing two or three weeks in intensive care before they eventually go on a ventilator. Once that happens, 95 percent die.
If everyone could see what she sees, she says, the horror and hopelessness her nurses live with every day, the anguish the patients’ families endure, maybe they’d believe.
6:35 a.m.
How did you decide on using time as part of the narrative structure?I did that for my own edification when I was making a timeline and it just kind of stuck. I kept tracking which were the most important moments during the first couple of hours. Then I just found myself putting timestamps in there.After the woman in Room 84 is sedated and someone sends her son home, after a nurse rolls away the emergency cart, after Jen checks on an 80-year-old man from an assisted living facility, she sinks into a chair at the nurses’ station and opens a three-ring binder.
The night nurse manager peers over the pages with her, reports on each patient.
“This one with the belly bleed is unresponsive,” says the nurse. “Too fragile to move.” Jen nods. The nurse turns the page. “This girl in 93, doctors were trying to hold off for her, but ... "
Jen doesn’t look up. Now that the patients are staying longer, the nurses get to know them, and their families.
Jen knows the 36-year-old woman has two young children, that she’s been holding on for two weeks, that yesterday she had respiratory failure and turned blue.
“She’s going to need to be intubated,” the nurse says. The beginning of the end.
The ward is shaped like a U, with nine rooms on each side. The front walls are glass, so staff can see into them without opening the doors. The ventilation system has negative pressure, so contaminated air recirculates into the ducts.
Most of the patients are motionless, sunken into medical comas. The few who are still conscious sometimes moan.
TVs are not on here. There’s no music. No visitors, until the end. But nurses constantly call out to each other, phones ring, the halls buzz and beep. And too often, a siren screams throughout the hospital, blue lights spin from the ceiling, signaling someone has coded -- if not already died.
Nurses have little time to put things in perspective or process the pain. There’s a massage chair in the break room, piles of granola bars and cheese sticks. But they often skip meals.
A poster by the medicine room proclaims: Here’s to another day of outward smiles and inward screams.
When you first saw this poster did you recognize its significance to the story?Yes, absolutely. I’m always reading the walls, looking for signs and stories and cartoons and bumper stickers and memes. What do people put up around them? I feel like that gives you a really good insight into how they see themselves or what they use to motivate themselves. That’s always one of the first things I’m doing — scanning the walls of the bulletin boards.
8:00 a.m.
The man in Room 89 is deteriorating. His lungs blew out from pumping so much oxygen into them. Doctors put him on steroids, and he’s been on a ventilator for two weeks.To relieve pressure on his lungs, he needs to be flipped over, onto his stomach, the respiratory therapist says. The patient is hooked to a tangle of tubes and a half-dozen monitors. He’s a big man. Most of the people in this ward are obese.
He’s 50 years old — the same age as Jen.
“I’m coming,” she calls, pulling on blue gloves and her N95 mask. “Hey, we need another pair of hands.”
How did you determine which details to focus on and how much time to spend observing Jen versus exploring the ICU on your own?I was very confused to tell you the truth. The whole thing was exhausting. I didn’t know if I was getting what I needed. John Pendygraft, the photographer, and I split up as often as we were together. He would see something in one place and alert me and I would see something and alert him. He was trained on Jen a lot while I was trying to ask the other people in the hall what was going on.
Six people work together to roll sheets beneath the patient and thread tubes out of the way. Jen stands by his head as a co-worker pulls out the ventilator, watching the numbers dropping on the monitor. Two more nurses are “bagging” the man, manually pumping air into his lungs until they can reconnect the machine.
Once he’s turned, Jen re-hooks his lines, smooths a clean sheet over his back, checks to see if his vital signs improve.
They don’t. Ten minutes later, he’s worse than when he was on his back. Jen shakes her head and tells the nurse beside her, “He’s not going to make it out of here.”
8:30 a.m.
Rounds are supposed to start at 8 a.m. But with so many emergencies, they often begin late.The team gathers in the hall, a dozen people: Nurses, therapists, doctors. A pharmacist. A chaplain. A social worker. A dietician. A couple of interns. They each push a cart with at least one laptop on it, checking information, typing into charts.
Jen carries two phones and a beeper and wears an Apple watch to check email. Sometimes, nurses on other floors need her. Sometimes, she needs help, with X-rays, prescriptions, tests and specialists.
“It’s a little crazy in here,” a nurse tells the primary doctor on duty.
“Not as bad as yesterday,” he says. Not yet.
Outside each room, a nurse reads through a chart, updating the team on the patient’s condition. They talk about family members: Who is making medical decisions? If they can’t find a relative, they go through the patient’s phone.
They start rounds at Room 81, where the man’s stomach is bleeding. “He’s not doing well,” the nurse says.
They’re about to head to the next room when Jen interjects, “The woman in 84 is really looking bad.”
So the team heads across the hall. “After you get a PICC line in, try to prone her,” the doctor says, meaning they should roll her onto her stomach.
“Who is her health care surrogate?” asks Jen. “We need someone legally to make some decisions.”
In Room 86: A 46-year-old man got so aggressive he had to be sedated.
Room 91: This man has been in the ICU for a week. “Very anxious,” says a nurse.
On the way to the next room, Jen’s cell rings. “Yes, we just got a new one. No, we don’t have a bed,” she tells a nurse on another floor.
Room 92: Jen says of this woman, “There’s not much more we can do.”
Room 95: This woman has pneumonia, almost coded yesterday.
Room 97: The man was hypothermic overnight.
On other floors, seven more COVID-19 patients are waiting to get into the ICU.
A doctor, who had been on duty the day before, walks up to Jen on his way through the ward. “Hey, are you okay?” he asks. “I was thinking about you last night.”
Jen swallows and nods without meeting his eyes.
There is so much vivid detail, yet repressed emotion in this story. Did you get that feeling as you were reporting?There was a little bit of conversation among the nurses, but it was mostly about the patients. They were these stoic, front-line emergency workers and they’ve dealt with this shit every day and they were getting overwhelmed and exhausted, but they weren’t really letting themselves get too emotional. They couldn’t afford to. I felt like they were more trying to buck up each other than letting themselves feel a lot of stuff.
10:50 a.m.
After hours on her feet, Jen finally gets to sit. At the nurses’ station, she reads lab reports, answers calls, talks to families.Someone brings Publix subs to the ward, so she takes a few bites in the break room before her beeper goes off again.
A man who had been intubated on a ward upstairs has gone downhill. His family has decided to withdraw care. Instead of coming to the ICU, he will be going to the morgue.
This was one of several passages where you presented disquieting revelations about death inside the ICU using a series of punchy sentences. How did you decide the ways you would describe the suffering you witnessed?Each one struck its own little hammer beat. It was there and it was over and it was there and it was over. I try, sometimes, to fast forward through hard parts. Instead of making somebody drown in the misery, just hammer it quick and back off. I think sometimes that’s more effective than making you go into the black hole and have to climb back out.
“He was here with us before,” Jen tells a nurse. “We transferred him out. But … "
By the time most patients come to the ICU, their bodies are exhausted from struggling so hard to breathe. Their hearts are deprived of oxygen, so their blood pressure plummets. They’re in pain and panicking.
Nurses try to make them comfortable and update their loved ones.
When you can’t see the patient, you don’t know how bad things are. You don’t realize, or admit, Jen says, when it’s time to let go.
The nurses don’t want to prolong anyone’s suffering, Jen says. “But we do it until the family is ready to stop.”
When death seems imminent, one visitor is allowed in the room. If there’s no relative or friend, a nurse holds the person’s hand. “No one dies alone here,” Jen says.
Some patients have Do Not Resuscitate orders: If they stop breathing, or their heart gives out, they don’t want CPR. But those orders don’t necessarily include ventilators, Jen says. Over the last couple of years — mostly since COVID-19 — health care officials have required a new classification: Do Not Intubate.
Most people don’t know they need that, Jen says.
Just before noon, she ducks into Room 85. The man from assisted living is doing so much better he can be transferred to another floor. He’s the oldest person on her ward, the only one who got the vaccine.
At any point, did you all take a break from reporting?Full disclosure: We didn’t spend the full 12 hours inside the ICU. They kicked us out because they said that staff and Jen needed a break. We were (scheduled to be) there from 6 a.m. to about noon and then 2 p.m. to about 6 p.m. For the two hours in the middle, they made us not only leave the ICU, they made us leave the hospital because they didn’t want us bothering people in the cafeteria. John and I just left and got a pizza and spent the whole time going, “What the ----? What are we missing?” John and I came back early at 1:30 instead of 2 p.m., and we’re waiting in the lobby for the PR person from the hospital to come back and take us upstairs. The president of the hospital comes down off the elevator and he goes, “Oh my God, the woman in Room 84 is coding. You’ve got to get up there. Go, go, go.” I was able to report right at that moment and Jen was like, “Yeah, you missed nothing between 12 and 1:40.”
2:35 p.m.
Blue lights flash overhead. A siren howls.Jen and her team rush to Room 84. Around the patient, two doctors and five nurses are pumping medications through IVs, trying to keep oxygen circulating to her organs.
A machine, the size of a shoebox, is strapped across the woman’s chest. The “Lucas 3” device is new, a product of the pandemic, and does chest compressions so nurses don’t have to.
I noticed that Lucas, the machine, is the only name other than Jen’s who you present in the story. The remaining nurses and doctors are anonymous. Can you talk about this decision? There was a team of 16 or 18 people doing rounds and following these patients. I got all their names and titles and details about their kids and how many years they’ve been there. When I sat down to write it, I thought, “I can’t go into 16 different lives and names and nursing titles.” It really felt like it was mucking up the narrative. I kind of do this thing by default: I close my eyes. If I’m writing a story like I watch a movie, I wouldn’t need to know all those names and titles. I can flesh Jen out as a character. So I focused on her most of the time.
Each time it pushes, the woman’s body convulses, arms and legs jerking.
“Everybody knew it was going to come to this,” a nurse says from the hall.
Still, they try. And try again.
When the woman came in this morning, she had begged a nurse to do anything. Anything! Her son said the same thing: No matter what, don’t let her go.
“You gotta call him again,” Jen says.
Another nurse picks up her phone, dials the number on the whiteboard by the door. “Your mom has coded again,” she tells the son. “It’s really not looking good. At this point, we’ve given her all the medications we can.” She pauses. “I don’t know if you want us to continue to do this. You can come up to see her.”
The son is a 45-minute drive away. The nurse offers to FaceTime, but he has an Android phone.
“She’s failing, actively dying,” the nurse tells the son. “I’m sorry to say that to you. We’ve given her 110 percent. But she’s just spiraling back down ... I think at this point, it’s time to give her peace.” Silence.
“Do you want me to put a phone to her ear, so she can hear your voice?”
In the hall, through the glass, everyone hears her son weep.
Jen walks away. At the nurses’ station, she drops her head into her hands. She tries not to think about all the patients she’s lost, the children they won’t see grow up, the grandkids they’ll never know. How did you go about getting these interior details about Jen?When I take notes, I put arrows in the margins so I know where to go when I go back and ask follow-up questions. I wrote down a whole bunch while stuff was going on. There were questions I thought of in the moment, but I wasn’t able to interrupt her doing her job until she was able to slow down. I just peppered her with them when she would stop for a minute to check email. I was walking with her when she was walking to refill her water bottle. Any chance I got. “When this was happening what were you thinking?” or “Is it hard to not take this personally?” I was just getting snippets here and there. It was not ideal.
In Room 83, the family of a woman who has been in the ICU for 25 days has decided to take her off life support. She’s 56. A wife and mother.
Orderlies roll a new patient onto Jen’s ward. This woman is 54. She’s been in the hospital for three days. She’s wrapped in thick plastic, so she doesn’t expose others to the virus. She looks like she’s been swaddled in Saran Wrap. She needs to be sedated and put on a ventilator. Now.
As Jen hurries to meet her in Room 96, another nurse draws her into the coffee room. “Here, you need to eat,” she says, shoving a fork toward Jen’s mask.
For the first time all day, Jen laughs.
This nugget: Were you keeping track to see if this was the first time she laughed, or did you ask Jen directly?Both.
“There’s nothing like eating a tamale, then putting on an N95,” she says. “Yummy!”
3:20 p.m.
The woman in Room 84 codes again. Lights. Sirens. A dozen people rush to the room.“We gotta stop. We’re not doing anything for her,” says a nurse.
“Her son says he’s on the way,” says another. “He wants us to keep her alive until he can say goodbye.”
In Room 89, the man they had rolled over had his chest tube pop out. Jen sends someone to reinsert it. In Room 95, a woman’s daughters have decided to let her go.
Then the woman in Room 84 codes again.
Every 20 minutes, the staff brings her back.
She has now coded seven times.
“This is something we don’t do,” Jen says.
Jen’s not religious or spiritual. She doesn’t ask why things happen, what they mean. Or what comes after death. She’s cemented in the here and now, multi-tasking through every moment. Making life and death decisions.
Finally, the woman’s son runs in. Two nurses help him put on a gown, gloves, mask and goggles. “Would you like the chaplain to be here with you?” asks a nurse.
The son looks stunned. He swallows, blinks back tears, nods.
Were you allowed to follow up with any of the patients’ families after witnessing these events in the ICU?No, not at all. In fact, they didn’t even want the patients’ families to know we were there, so when the son came to see his mom in Room 84, we kind of had to scoot around the side where we weren’t visible. You know, we had done so many other stories from the patients’ and patients families’ points of view, I was OK with just doing the nurses’ story.
He shuffles into the room, freezes and stares. Then he collapses on top of his mother.
Through the door, Jen motions for a nurse to unstrap the machine that’s keeping her alive.
So her son can truly hug her.
Did you start to react to the pain as you watched these moments unfold?In the moment, I was so worried about getting everything I could and getting it right and not missing anything and swiveling and working within the parameters and understanding what was going on that I wasn’t really letting it sink in. I didn’t cry about it until I started to write.
5:50 p.m.
Near the end of her shift, Jen’s back is sore. Her knees ache. She’s thirsty. No time to fill her water bottle. She keeps yawning.She can’t stop thinking about the man who just lost his mom, and her own mom, who she lost in June to cancer.
A nurse from another COVID-19 ward comes to see Jen. She lost two people today and had heard ICU did, too. The nurses embrace, feeling each other’s pain.
For the next half-hour, Jen works on scheduling, checks on her nurses, walks the ward one more time.
When the night nursing supervisor comes, she briefs her on each patient.
Room 83: She’s CMO. Comfort Measures Only.
Room 84: The woman finally passed. But her son is still with her.
Room 86: This man brought pictures of his family. He told the ER nurse: Don’t let me die.
Room 89: He’s still prone, still struggling. He’s got kids. He’s not going to make it.
“But 93 is better, right?” asks the night nurse, referring to the young mom.
Jen drops her eyes and says softly, “Nooooo.”
What did you have to cut from the piece that you wish could have appeared in print?I had a lot more about the one young woman who had little kids. To me, she was one of the ones they were all rooting for the most and maybe the one who had the most to lose. (The PR staff) made me strip so much detail about her that I felt like she ended up being not even a secondary character. And I really wish I had that hour-and-a-half in the middle of the day when they kicked us out to be there when Jen finally took a bite of a sandwich or when they finally got to sit down and breathe for a minute. I regret that I couldn’t get to Jen directly to call her at night. Some of my favorite interviews are through after-the-fact debriefing or fact checking when it’s late at night. You can just be, “Oh my God, what happened today?”
Saving sick people used to motivate her to keep doing this hard work. Now, she says, there’s no joy to buoy her through the sorrow. “You wonder: How long can I do this for?” she says. “I’ve definitely thought about what I want to do next. I want to work with dogs.”
She’s grateful for her own health, her friends’ and families’ health. And that she finally convinced her 18-year-old son to get the shot. “I had to bribe him with $100,” she says.
She’s incredulous at co-workers who won’t get vaccinated. BayCare doesn’t require its employees to, but it asks each patient.
For a while, the community was cheering for health care workers, bringing so many meals they donated some to the food bank. This summer, the love seemed to evaporate. On the “Heroes Work Here” sign, someone added the word “Still.”
“I don’t feel like a hero,” Jen says. “I feel helpless.”
To me, there is a bittersweet balance to this story. On one hand it conveys the resilience of front-line workers, but also the senseless tragedy of dragging them through what feels like an exercise in futility. Yet, you are known for attempting to find threads of hope in your stories. Were you able to locate them?Jen just kept saying, “I don’t have any.” (But) if you chose to go into this profession, you basically push yourself to do whatever you can to make strangers’ lives as bearable as possible. Whether you’re in a pandemic or a car crash or a mass shooting, these are the people that are going to be there. Jen or any of those other people could quit at any time. It’s duty but it’s also love. There is something to hang onto there.
6:10 p.m.
Like most of the nurses, Jen will drive home in silence.Some try to process their day, so they don’t take it to their families. Others try to block it out, so they don’t have to relive it.
Jen tries to not think about anything during her commute to Palm Harbor, which, of course, is impossible. When she gets home, she works out or walks her two dogs.
What was your ride home like? What did you tell your family when they asked how your day was?John and I rode to this story and back together. I really like being there with the photographer to plan and debrief. John is a very loquacious and very intelligent and very deep-thinking person, but the whole way back he didn’t say one word. Like the nurses, we didn’t really want to talk. You just had to process what happened, both in the reporting and the emotional toll. That could be my mom or my friend or my coworker. I’ve watched people die before, but I don’t think I watched three people die in a day. I came home and had a glass of wine and my husband was like, “How did it go?” I was like, “Mmm, I’m really, really exhausted. How was your day?” I didn’t want to rehash it all. But also, I don’t want to sit there and say I had a hard day because then I think that’s Jen’s day every day. I get to work from my home in my yoga pants tomorrow. She’s got to be back in there at 5:45 a.m. and do that all over again.
Her kids don’t ask about her day much. Her husband pours her a Chardonnay and lets her talk -- if she wants.
He doesn’t understand why she’s putting herself through this.
But this job is what she does. And who she is.
She can’t walk away. Not now.
How did readers react to your story?I got hundreds of emails. At least a third were from health care workers or family members of health care workers who were like, “Thank you so much for telling people what it’s like in there.” And some from some nurses who were like, “I couldn’t take it anymore. I quit last month.” And you could tell they felt guilt, that they had bailed while Jen was still in there fighting the fight. Answering those emails was really hard. But the best aftermath of the story was that two readers emailed me and said because of your story my spouse went and got the vaccine. I did not hear from Jen directly, but the PR staff said the nurses were very grateful. A bunch of local restaurants and delis sent food and lunches and bagels and breakfasts and smoothies to the nurses. A girl who is in ninth grade sent them thank-you notes. Our governor, Ron DeSantis, unbeknownst to me, his mother was an ICU nurse. One of her former coworkers wrote to thank me and said, “I just mailed your story to our governor. How could he do this when his mother was an ICU nurse for 30 years?”
*** Bennet Goldstein is a general assignment and features reporter at the Dubuque (Iowa) Telegraph Herald.